Whole Secret – Whole Fantasy: The US-China relationship is just a “Fantasy” for the adulterous relationship began without taking into consideration the fact of Tibet’s legitimate presence in the global community of nations.
In my analysis, the US-China relationship is just a ‘Fantasy’ for the adulterous relationship began without taking into consideration the fact of Tibet’s legitimate presence among the global community of nations.
Whole Secret – Whole Fantasy: The US-China relationship is just a “Fantasy” for the adulterous relationship began without taking into consideration the fact of Tibet’s legitimate presence in the global community of nations.
Rudra Narasimham Rebbapragada
SPECIAL FRONTIER FORCE
Whole Secret – Whole Fantasy: The US-China relationship is just a “Fantasy” for the adulterous relationship began without taking into consideration the fact of Tibet’s legitimate presence in the global community of nations.
Where Does Tibet Fit Into the US-China Relationship? | The Diplomat
Whole Secret – Whole Fantasy: The US-China relationship is just a “Fantasy” for the adulterous relationship began without taking into consideration the fact of Tibet’s legitimate presence in the global community of nations.
Image Credit: Flickr/ Laika ac
With the U.S. ambassador’s visit, Tibet may again be poised to play a larger role in US-China relations.
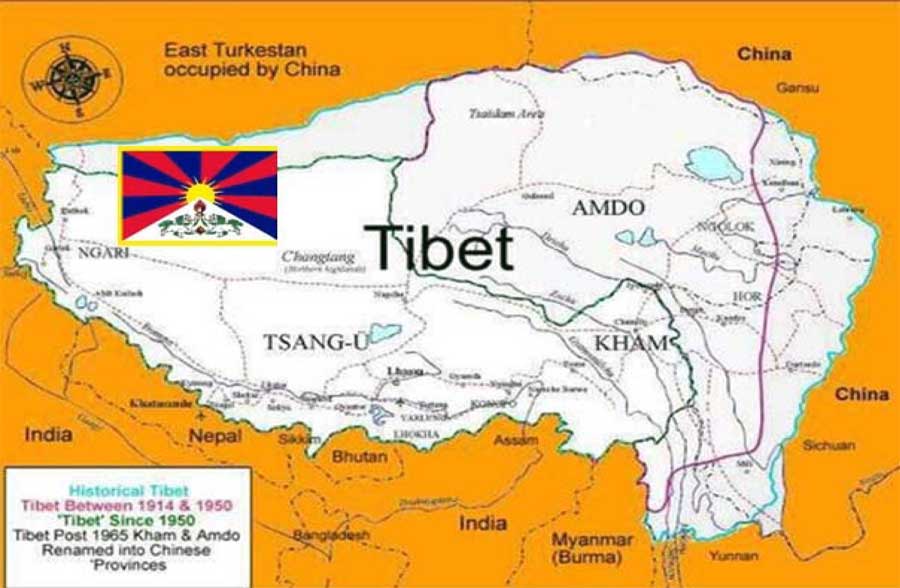
Through May 25, U.S. Ambassador Terry Branstad is on a rare visit to Tibet, the first by a U.S. envoy to the Chinese autonomous region since 2015. His trip includes official meetings and stops at religious and cultural sites in bid to raise concerns about religious freedom restrictions and cultural and linguistic preservation, according to the State Department.
Tibet, geographically on China’s western flank, is a gateway to South Asia, and has been a perennial source of political sensitivity for Beijing. China’s trepidation over foreign influence and the U.S. connection to Tibet is not completely unfounded. Prior to the normalization of China-U.S. relations, the CIA funneled funding to the Dalai Lama — an influential spiritual leader of Tibetan Buddhism now exiled in India — and the Tibetan community to support covert activities against China. The program was canceled as then-President Richard Nixon set off on his landmark trip to Beijing in 1972. Since then, U.S. ties to Tibet have been kept more at an arm’s length, with periodic calls for the upholding of individual rights broadly and the provision of aid to safeguard Tibetan identity. And over the past year, Beijing’s approach to Tibet has attracted less attention in the United States than the Chinese government’s expansive security policies in neighboring Xinjiang, another nominally autonomous ethnic region in China.
The ethno-religious identity and status of Tibetan Buddhists lies at the heart of tensions between central authorities, the local government, and the local population. While the region is administered by the People’s Republic of China, China’s sovereign claim is contested by some groups. Beijing traces is control back to the rule of the Ming and Qing dynasties, and of course a 1951 agreement that declared Tibet’s “peaceful liberation”; others hold that the People’s Liberation Army invaded and occupied the territory. Under Beijing’s administration, religious and other activities are restricted to quell and thwart dissent and uprisings. Although detention centers have been piloted in Xinjiang, Tibet is also subject to heightened cybersurveillance, a repertoire of surveillance and repression by authorities, and the promotion of Han Chinese migration and mixed marriages to the region to bolster “national unity.”
This week’s high-profile U.S. visit in Tibet may be appealing to both Beijing and Washington, albeit for different reasons. Certainly, both are looking to frame their relationship in terms that extend beyond trade disagreements as the latest round of bilateral negotiations crumbles. A successful trip in Beijing’s eyes will highlight the coexistence of Han Chinese and Tibetans, the modernization of Tibet, and initiatives to support Tibetan culture, language, and Buddhism; a stark contrast from Beijing’s policies toward Muslim communities in neighboring Xinjiang. Conversely, for Washington, this trip can be viewed as a move by the Trump administration to demonstrate the U.S. commitment to protecting human rights, a facet of Trump’s foreign policy that has been criticized, notably in the context of U.S.-China relations.
However, it may be hard to disentangle the actual motivations for the Tibet visit. Instead, the Trump administration, frustrated by the state of trade negotiations, may be taking a more instrumental position toward Tibet and using it to indirectly pressure Beijing over a political charged region. Even if the trip is motivated by a desire to raise rights awareness, one visit to Tibet by Branstad is unlikely to overturn criticisms that the Trump administration is reluctant to center human rights issues as a key component of the U.S.-China relationship. This criticism has been voiced both by international rights watchdogs, like Human Rights Watch, and from bipartisan members of the U.S. Congress, frustrated by the executive branch’s slowed actions. Washington, once a pioneer on these issues, has ceded its international leadership role under the current administration in favor of issuing human rights criticisms more selectively.
With respect to Tibet, some have expressed concern that China’s growing international power may have dampened support and narrowed the political space for the “Free Tibet” movement. Still, the United States passed the Reciprocal Access to Tibet Act in late 2018, which would require the U.S. government to punish officials who restrict access to Tibet for U.S. diplomats, journalists, academics, and other citizens traveling to the region. Although the law may unintentionally lead to a dip in visits by Tibetan delegations to the United States, the ratcheting up of pressure may possibly nudge China to review the ways in which it accords access to Tibetan areas.
Nevertheless, it remains to be seen if Tibetans will stand to benefit from the temporary diplomatic spotlight brought by Branstad’s brief tour.
Whole Secret – Whole Fantasy: The US-China relationship is just a “Fantasy” for the adulterous relationship began without taking into consideration the fact of Tibet’s legitimate presence in the global community of nations.Whole Secret – Whole Fantasy: The US-China relationship is just a “Fantasy” for the adulterous relationship began without taking into consideration the fact of Tibet’s legitimate presence in the global community of nations.
Doomed American China Fantasy – The Cold War in Asia
DOOMED AMERICAN CHINA FANTASY – THE COLD WAR IN ASIA 1949 TO 2026. THE SPREAD OF COMMUNISM IN ASIA.
The Cold War in Asia is the product of Communism that spread from Europe to Asia. Nixon-Kissinger in 1971-72 initiated Policy of Doomed American China Fantasy without concern for lessons learned in Korean Peninsula and Vietnam. There is no hope and there is no future for America’s China Fantasy as Communist Party in China survives unchanged and unaffected by changing fortunes of the US Political Parties.
Rudra Narasimham Rebbapragada
DOOM DOOMA DOOMSAYER
Doomed Gun of Doom Dooma symbolizes the Doomed China Fantasy, a Policy initiated by 37th US President Richard M Nixon when he made a trip to Peking on February 21, 1972. DOOMED AMERICAN CHINA FANTASY – THE COLD WAR IN ASIA 1949 TO 2026. THE SPREAD OF COMMUNISM IN ASIA.DOOMED AMERICAN CHINA FANTASY – THE COLD WAR IN ASIA 1949 TO 2026. THE SPREAD OF COMMUNISM IN ASIA. DOOMED AMERICAN CHINA FANTASY – THE COLD WAR IN ASIA 1949 TO 2026. THE SPREAD OF COMMUNISM IN ASIA.
AMERICA’S CHINA FANTASY
DOOMED AMERICAN CHINA FANTASY – THE COLD WAR IN ASIA 1949 TO 2026. THE SPREAD OF COMMUNISM IN ASIA. President Nixon’s Doomed Journey to Peking in February 1972.
America has been operating with the wrong paradigm for China. Day after day, U.S. officials carry out policies based upon premises about China’s future that are at best questionable and at worst downright false.
The mistake lies in the very assumption that political change — and with it, eventually, democracy — is coming to China, that China’s political system is destined for far-reaching liberalization. Yet the Bush administration hasn’t thought much about what it might mean for the United States and the rest of the world to have a repressive one-party state in China three decades from now. For while China will certainly be a richer and more powerful country in 30 years, it could still be an autocracy of one form or another. Its leadership (the Communist Party, or whatever else it calls itself in the future) may not be willing to tolerate organized political opposition any more than it does today.
That is a prospect with profound implications for the United States and the rest of the world. And it is a prospect that our current paradigm of an inevitably changing China cannot seem to envision.
The notion of a China on the road to political liberalization has taken hold in the United States because it has served certain specific interests within American society. At first, in the late 1970s and the 1980s, this idea benefited the U.S. national-security establishment. At the time, the United States was seeking close cooperation with China against the Soviet Union, so that the Soviet Union would have to worry simultaneously about both countries; the Pentagon wanted to make sure the Soviet Union tied down large numbers of troops along the Sino-Soviet border that might otherwise have been deployed in Europe. Amid the ideological struggles of the Cold War, though, cooperation with China’s Communist regime was politically touchy in Washington. And so the notion that China was in the process of opening up its political system helped smooth the way with Congress and the American public.
In the 1990s, after the Soviet collapse, the idea of a politically changing China attracted a new constituency, one even more powerful than the Pentagon: the business community. As trade and investment in China became ever more important, American companies found themselves repeatedly beset with questions about why they were doing business with such a repressive regime. The paradigm of inevitable change offered multinational corporations the answer they needed. Not only was China destined to open up its political system, but trade, the theology held, would be the key that would unlock the door. It would lead to political liberalization and to democracy, with or without the support of the Chinese leadership. Accordingly, no one outside China needs to do anything, or even think much about the subject. Why bother to protest a crackdown or urge China to allow political opposition if you know that democracy, by the inexorable laws of history, is coming anyway?
The trouble is, the entire paradigm may turn out to be wrong.
What should the U.S. strategy be for dealing with China’s Leninist regime? If you ask our established political leaders, foreign-policy experts, or sinologists what the United States should do about China, you will undoubtedly get some version or another of this approach. It is called the strategy of “integration.”
The United States, the thinking goes, should try to integrate the Chinese leadership into the international community. It should seek to help China gain admission into the world’s leading international organizations. According to this logic, the nature of the Chinese regime will change after China becomes a member of international bodies such as the World Trade Organization, which it has now joined. China’s Communist Party leadership will gradually behave more like other governments; it will become more open in dealing with the Chinese people and with the rest of the world. Richard Haas, the president of the Council on Foreign Relations, has written of “the existing opportunity to integrate China into a U.S.-led world order.”
This strategy of integration dates back to the Clinton administration. In 1994, President Clinton abandoned his attempt to use trade as a lever for improving human rights in China, then needed to divert attention away from this embarrassing reversal. He did not wish to concede that that he had just downgraded the cause of human rights in China; instead, he sought a new, positive-sounding description of his policy. “Integration” gradually became the label of choice, invoked by the president and his top advisers in press conference after press conference. Integration became, above all, the justification for unrestricted trade with China. “We believe it’s the best way to integrate China further into the family of nations and to secure our interests and our ideals,” declared Clinton in one typical speech.
George W. Bush and his advisers, without ever admitting they were doing so, have perpetuated most of the essentials of Clinton’s China policy, including the avowed commitment to integration. When Secretary of State Condoleezza Rice gives a speech about China, she sooner or later calls for integrating China into the international community.
“Integration” has thus become another catchphrase like “engagement,” the earlier slogan for America’s China policy, which originated somewhat earlier, during the administration of George Bush Senior. With both words, however, the suggestion is the same: that is, with enough engagement, with sufficiently vigorous integration, the United States may succeed in altering the nature of the Chinese regime — although it is not clear exactly how this is supposed to happen. In a way, the American approach is a bit patronizing to China: It sounds as if the United States is a weary, experienced trainer bringing China to a diplomatic version of obedience school.
The fundamental problem with this strategy of integration is that it raises the obvious question: Who’s integrating whom? Is the United States now integrating China into a new international economic order based upon free-market principles? Or is China now integrating the United States into a new international political order where democracy is no longer favored, and where a government’s continuing eradication of all organized political opposition is accepted or ignored?
This is not merely a government issue. Private companies — including Internet firms like Yahoo, Google, and Microsoft — often use slogans like “engagement” and “integration” to explain why they have decided to do business in China despite Chinese rules and laws that allow continuing censorship. “I think [the Internet] is contributing to Chinese political engagement,” Bill Gates told one business gathering. Yet if Microsoft is altering its rules to accommodate China, once again the question is: Who’s changing whom?
Will it have been a success for the U.S. policy of integration if, 30 years from now, the world ends up with a Chinese regime that is still a deeply repressive one-party state but is nevertheless a member of the international community in good standing? If so, that same China will serve as a model for dictators, juntas, and other undemocratic governments throughout the world — and in all likelihood, it will be a leading supporter of these regimes. Pick a dictator anywhere today and you’ll likely find that the Chinese regime is supporting him. It has rewarded Robert Mugabe, the thug who rules Zimbabwe, with an honorary professorship, and his regime with economic aid and, reportedly, new surveillance equipment. It has been the principal backer of the military regime in Burma. And when Uzbek President Islam Karimov ordered a murderous crackdown on demonstrators in 2005, China rushed to defend him.
If China maintains its current political system over the next 30 years, then its resolute hostility to democracy will have an impact in places like Egypt, Syria, and Saudi Arabia. A permanently authoritarian China could also undermine Russia’s already diminishing commitment to democracy.
Thus, when America’s leading officials and CEOs speak so breezily of integrating China into the international community, listeners should ask: If China remains unchanged, what sort of international community will that be? Will it favor the right to dissent? Will it protect freedom of expression? Or will it simply protect free trade and the right to invest?
But wait, say the defenders of America’s existing China policy. We believe in democracy, too. There is no real disagreement here on our ultimate goals. This is all just a question of tactics. The strategy of integration (or of engagement) is designed to change China’s political system and, over the long term, to end China’s one-party state.
These arguments sound in some ways similar to claims made by the Chinese regime itself. Because Chinese Communist Party leaders don’t like to acknowledge that they intend to maintain their monopoly on power, they sometimes tell visitors that they, too, believe in democracy, that this is the ultimate goal for China, and that it is all merely a question of timing. These claims are designed for the hopelessly gullible; by its actions, day after day, the regime makes clear its tenacious hostility to the idea of political pluralism in China.
Generally, the U.S. proponents of a strategy of integration are not so cynical. To be sure, a few of them may be antidemocratic; there have always been Americans who admire, even revere, the simplicity and convenience of autocracy. However, other proponents of integration seem to believe quite sincerely that if the United States continues its current approach toward China, Chinese leaders eventually will be willing to abandon the monopoly on political power they have maintained since 1949. Yet these same proponents fail to explain how or why, given the current U.S. strategy, China’s political system will change.
The examples of reforms that they have invoked so far have served to divert attention away from the core issue of China’s one-party state. The promotion of village elections has proved to be largely unsuccessful, both because the Chinese leadership can confine this experiment exclusively to the villages and because in the villages themselves, authorities have resorted to a variety of methods, including the use of violence, to forestall democracy.
Nor is there evidence that the American promotion of the rule of law will by itself transform the political system. So long as there is no independent judiciary and China remains a one-party regime in which judges are selected by the Communist Party, promoting the rule of law won’t bring about fundamental change. Instead, it simply may lead to a more thoroughly legalized system of repression. Indeed, those lawyers in China who attempt to use the judicial system to challenge the Communist Party or to defend the rights of political dissidents have themselves been subject to persecution, including the loss of their jobs or even time in prison.
The strongest impetus for establishing the rule of law comes from the corporations and investors who are putting their money into China. They need bona fide procedures for resolving financial disputes, just as companies and investors require everywhere else in the world. It is in the interest of the Chinese regime to keep the investment dollars, euros, and yen flowing into the country, and so Chinese officials are willing to establish some judicial procedures for the foreign companies. However, the result could well be a Chinese legal system that offers special protection for foreign investors but not to ordinary Chinese individuals, much less to targets of the regime such as political dissidents or Tibetan activists.
And that raises the larger question about America’s current strategy of integration: Whom does it benefit? Above all, it enriches the elites in both China and the United States. The strategy is good for the American business community, which gets to trade with China and invest in China, and for the new class emerging in Chinese cities — the managers and entrepreneurs, many of them former party cadres or the relatives of cadres — that is getting rich from the booming trade and investment in its country. But it has not been nearly so beneficial for working-class Americans — particularly the tens of thousands who have lost their jobs in the United States as the end result of this “integration” policy.
The American people were told many years ago that bringing China into the international economic system would help change the Chinese political system. Now, American workers may well wonder whether this argument was merely a cruel hoax. Nor has the strategy of integration been such a blessing for ordinary Chinese. To be sure, China as a whole is more prosperous than it has ever been, but this new prosperity is enjoyed mostly by the urban middle class, not by the country’s overworked, underpaid factory laborers or by the hundreds of millions of peasants in the countryside.
Indeed, it is precisely because the regime knows how restive and disenchanted the Chinese people are that it refuses to open up to any form of democracy. The Chinese leaders know that they could be thrown out of office if there were free and open elections. Democracy, or even an organization calling for future democracy, is a threat to the existing political and economic order in China. That is why the regime continues to repress all forms of organized dissent and political opposition. It is also why China’s new class of managers and executives, who profit from keeping wages low, support the regime in its ongoing repression.
A few years ago, the New York Times columnist Nicholas D. Kristof gave voice to one of the most common American misconceptions about China’s political future. Reflecting on how China had progressed and where it was headed, Kristof wrote, “[Hard-liners] knew that after the Chinese could watch Eddie Murphy, wear tight pink dresses and struggle over what to order at Starbucks, the revolution was finished. No middle class is content with more choices of coffees than of candidates on a ballot.”
Once people are eating at McDonald’s or wearing clothes from The Gap, American writers rush to proclaim that these people are becoming like us, and that their political system is therefore becoming like ours. But will the newly enriched, Starbucks-sipping, condo-buying, car-driving denizens of China’s largest cities in fact become the vanguard for democracy in China? Or is it possible that China’s middle-class elite will either fail to embrace calls for a democratic China or turn out to be a driving force in opposition to democracy?
China’s emerging urban middle class, after all, is merely a small proportion of the country’s overall population — far smaller than its counterparts in Taiwan or South Korea. There are an estimated 800 million to 900 million Chinese peasants — most of them living in rural areas, although 100 million or more are working or trying to find jobs as migrants on the margins of Chinese cities. If China were to have nationwide elections, and if peasants were to vote their own interests, then the urban middle class would lose. The margin would not be close. On an electoral map of China, the biggest cities — Shanghai, Beijing, Tianjin, Guangzhou, and the others — might look something like the small gold stars on the Chinese flag: They would be surrounded by a sea of red. Add together the populations of China’s 10 largest cities and you get a total of some 62 million people. That number is larger than the population of France or Britain or Italy. But it is still only about 5 percent of China’s overall population of 1.3 billion.
If you are a multinational company trying to sell consumer products, then the rapid rise in spendable income in China’s largest cities is of staggering importance. When it comes to any national elections, however, that new Chinese middle class is merely a drop in the bucket. Those in China’s urban avant-garde have every reason to fear that they would be outvoted.
China’s urban residents have an even greater reason to fear democracy: The Communist Party has not exactly been evenhanded in its treatment of urban residents vis-à-vis peasants. On the contrary: Its policies have strongly favored the cities over the countryside. This is why there has been a wave of protests in the countryside, arising out of land seizures, local taxes, disputes over village elections, and similar controversies. It is also why the Chinese regime has been, in recent years, particularly fearful of mass movements that might sweep through the countryside and undermine the Communist Party’s control. Looking at Falun Gong, the quasi-religious movement that began to take hold during the 1990s, the Chinese leadership was haunted by a specter from the past: the Taiping Rebellion, which swept out of middle China in the 19th century and shook the Qing Dynasty to its foundations.
What lies behind the Chinese Communist Party’s monopoly on power and its continuing repression of dissent? The answer usually offered is the Communist Party itself — that the party and its more than 70 million members are clinging to their own power and privileges. This is certainly part of the answer, but not all of it. As China’s economy has thrived in recent years, strong economic and social forces have also emerged in Chinese society that will seek to protect the existing order and their own economic interests. The new middle class in Chinese cities is coming to favor the status quo nearly as much as does the Communist Party itself.
Why do we assume that what follows the Chinese Communist Party’s eventual fall will necessarily be political liberalization or democracy? One can envision other possibilities. Suppose, for example, that the party proves over the next decade to be no better at combating the country’s endemic corruption than it has been over the past decade. Public revulsion over this corruption reaches the point where the Chinese people take to the streets; leaders find they cannot depend on troops to quell these demonstrations; the Communist Party finally gives way. Even then, would the result be Chinese democracy? Not necessarily. China’s urban middle class might choose to align itself with the military and the security apparatus to support some other form of authoritarian regime, arguing that it is necessary to do so in order to keep the economy running.
The underlying premise of the U.S. integration strategy is that we can put off the question of Chinese democracy. But two or three decades from now, it may be too late. By then, China will be wealthier, and the entrenched interests opposing democracy will probably be much stronger. By then, China will be so thoroughly integrated into the world financial and diplomatic systems that, because of the country’s sheer commercial power, there will be no international support for any movement to open up China’s political system.
What should the United States do to encourage democratic change in China? A detailed list of policies can emerge only after we first rid ourselves of the delusions and the false assumptions upon which our China policy has long been based.
Above all, we have to stop taking it for granted that China is heading inevitably for political liberalization and democracy. President Bush has continued to repeat the American mantra about China, every bit as much as did his predecessors. “As China reforms its economy, its leaders are finding that once the door to freedom is opened even a crack, it cannot be closed,” Bush declared in one typical speech. Such words convey a heartwarming sense of hopefulness about China, but they do not match the reality of China itself, where doors are regularly opened by more than a crack and then closed again.
America’s political and corporate leaders also need to stop spreading the lie that trade will bring an end to China’s one-party political system. This fiction has been skillfully employed, over and over again, to help win the support of Congress and the American public for approval of trade with China. Trade is trade; its benefits and costs are in the economic sphere. It is not a magic political potion for democracy, nor has it brought an end to political repression or to the Chinese Communist Party’s monopoly on power, and there is not the slightest reason to think it will do so in the future. In fact, it is possible that our trade with China is merely helping the autocratic regime to become richer and more powerful.
America’s current China policy amounts to an unstated bargain: We have abandoned any serious attempt to challenge China’s one-party state, and in exchange we have gotten the right to unfettered commerce with China.
What we need now, above all, are political leaders who are willing to challenge America’s stale logic and phraseology concerning China. We need politicians who will call attention to the fact that America has been carrying out a policy that benefits U.S. and Chinese business interests far more than it helps ordinary working people in either country.
The reexamination should apply to both U.S. political parties and to both poles of the ideological spectrum. On the Democratic left, we need people who will question the assumptions that it is somehow “progressive” to say that democracy doesn’t matter or that it will automatically come to China some day. Such views aren’t in the least bit progressive, liberal, or enlightened. Rather, they were developed by the Clinton administration to justify policies that would enable Bill Clinton to win corporate support. During the 1990s, there were other views concerning China within the Democratic Party — those of Nancy Pelosi, for example, and George Mitchell, who took strong stands on behalf of human rights in China. The Democrats rejected those alternative approaches a decade ago. They would do well to reexamine them now.
Within the Republican Party, we need political leaders willing to challenge the Business Roundtable mentality that has dominated the party’s thinking on China for so long. If Republicans really care about political freedom, then why should they allow U.S. policy toward China to be dominated by corporate interests while the world’s most populous country is governed by a single party that permits no political opposition? President Bush has been able to conceal his business-oriented approach to China behind a facade of hawkish rhetoric. Republicans should not allow this to happen again.
Once the United States finally recognizes that China is not moving inevitably toward democracy, we can begin to decide what the right approach should be. On the one hand, it’s possible that America may seek new measures to goad the Chinese leadership toward democratic change. America also might want to reconsider its doctrinaire adherence to free trade in dealing with China. On the other hand, it’s possible that the American people may decide that there’s absolutely nothing that the United States can or should do about a huge, permanently undemocratic, enduringly repressive China. Such an entity, a Chinese autocracy persisting into the mid-21st century, would cause large problems for U.S. policy elsewhere in the world. Nevertheless, after weighing the costs and benefits of trying to push for democracy in China, the United States could opt for a policy of sheer acceptance of the existing order.
The American people are not being given such options now, however, because the choices are not being laid out. American politicians of both parties talk regularly as if liberalization and democracy are on the way in China. But what if China remains an autocracy? At the moment, that possibility seems to be outside our public discourse. We need to change that in order to figure out what we want to do.
It would be heartening if China’s leaders proceed along the lines that America’s political leaders predict. It would be wonderful if China opens up, either gradually or suddenly, to a new political system in which the country’s 1.3 billion people are given a chance to choose their own leaders. While wishing for such an outcome, however, I will not hold my breath.
James Mann, from whose new book, The China Fantasy, this article is adapted, is author-in-residence at Johns Hopkins University’s School of Advanced International Studies.
DOOMED AMERICAN CHINA FANTASY – THE COLD WAR IN ASIA 1949 TO 2026. THE SPREAD OF COMMUNISM IN ASIA.Doomed American Fantasy – The Cold War in Asia 1949 to 2026. Communist Party of People’s Republic of China remains unaffected and unchanged by changing fortunes of the US Political Parties.Nixon-Kissinger in 1971-72 initiated Policy of Doomed American China Fantasy without concern for lessons learned in Korean Peninsula and Vietnam. There is no hope and there is no future for America’s China Fantasy
America’s China Fantasy from its very beginning in 1971-72 is destined to fail. Doomed American Fantasy – Read The Writing On The Made in China Label – Wake Up Call For America.
I was serving in Doom Dooma, Tinsukia District, Assam, India and a witness to the foreign policy initiative of the US President Richard M. Nixon in 1971-72 with which the Americans began to chase the illusion called ‘China Fantasy’. The American plan is doomed from its very inception for it involved the backstabbing of Tibet and overlooking the evil actions of the Communist regime in China.
Doomed Gun of Doom Dooma: China Fantasy Doomed on February 21, 1972 with 37th US President Richard M Nixon’s Visit to Peking.America’s China Fantasy from its very beginning in 1971-72 is destined to fail.
China is our greatest foreign policy issue. But neither Trump nor Biden have it right.
Xi Jinping’s China is fundamentally different from the past. Neither Donald Trump’s nor Joe Biden’s approach fully responds to that new reality.
Robert Robb, Arizona Republic
The most important foreign policy issue for the next American president will undoubtedly be relations with China. Unfortunately, neither Donald Trump nor Joe Biden have an approach grounded in reality, with a clear-eyed view of our national interests.
Ever since economic reforms were launched by Deng Xiaoping in the late 1980s, the bipartisan consensus was that the best approach to China was engagement. As China grew more prosperous and less insulated, the thinking went, economic liberalization could lead to political liberalization as well. Or, at a minimum, China could be a non-threatening participant in the world’s economy and affairs.
This was not as naive an expectation, or at least hope, as sometimes depicted today. There were examples of countries with authoritarian systems of state capitalism evolving into democracies with true market economies. South Korea is the most obvious example.
Indeed, a “peaceful rise” of China was one of Deng’s objectives. And that was the approach taken by his successors until current China strongman Xi Jinping.
Trump is using Biden’s support for China joining the World Trade Organization in 2001 against him. But, at the time, that was a prudent move and consistent with American interests as they were then perceived.
Xi’s China is different now
All this changed with Xi, who has jettisoned much of Deng’s approach to China’s development.
Deng believed in communal and rotating leadership. Xi has had himself appointed authoritarian-in-chief for life.
Xi is remaking China to return the Communist Party as the central focus of all life in the country. The government is to serve the party. And private businesses are to serve the government.
Markets are still used to allocate resources more efficiently than heavy-handed central planning. But there are no such things as truly private businesses in Xi’s China. Their ultimate purpose is to serve the interests of the party.
A “peaceful rise” has been abandoned. The purpose of trade is no longer principally to improve living standards. It is to increase the reach and leverage of the government and party. Militarily and diplomatically, China is seeking to dominate its region and intimidate other countries in the Asia-Pacific.
With Xi’s China, the expectations or hopes that underlay the engagement approach are a lost cause. External engagement isn’t going to change Xi’s China. Only domestic political upheaval that rejects Xi Thought will do that. And that doesn’t appear to be on the horizon.
The US should do 2 things differently
The reality of Xi’s China warrants an abandonment of the engagement approach. There should be two strategic objectives to a new approach to China.
►First, insulate the American economy from China to the maximum extent possible. Among foreign policy boffins, this is referred to as “decoupling.”
►Second, increase the military and diplomatic capacity of China’s neighbors, so every regional conflict involving China doesn’t automatically become a conflict with the United States. Our current role as the de facto security guarantor in the region isn’t in our best interests.
What Trump gets wrong on tariffs
Tariffs are one tool that could be used in decoupling. Trump has famously declared himself to be Tariff Man. And his administration currently has tariffs in place on roughly $370 billion worth of Chinese goods.
But decoupling isn’t the true strategic objective of Trump and his tariffs. Trump believes that the score between countries is kept by the balance of trade. The purpose of Trump’s tariffs is to serve as leverage to get China to purchase more American goods. Indeed, he reduced some tariffs and pulled the plug on others in exchange for a Chinese promise to do exactly that.
Biden gets engagement wrong
In an essay for Foreign Affairs magazine, Biden makes clear that he still believes in the engagement approach.
The principal problem with Trump’s approach, according to Biden, is that it is unilateral. Biden promises to create a coalition with allies to pressure China to change troublesome behavior in trade. But to continue cooperation with China on things where, as Biden puts it, “our interests converge.” He specifically mentions climate change, nonproliferation and global health security.
There is no such get-tough-on-China coalition to be had. There’s some spine in China’s neighbors. But none in the European Union, whose trade leverage would be necessary to get China’s full attention.
Trump’s instinct is to reduce the exposure of the U.S. to regional conflicts elsewhere. But he has no strategic vision about getting from here to there.
In his essay, Biden doubles down on the commitment to be the region’s security guarantor, a role whose risks vastly exceed the benefits to the United States.
Trump’s erraticism or Biden’s return to unproductive engagement. Sadly, that’s the choice.
Robert Robb is an editorial columnist for The Arizona Republic and azcentral.com, where this column originally appeared. Follow him on Twitter: @RJRobb
America’s China Fantasy from its very beginning in 1971-72 is destined to fail.Doomed Gun of Doom Dooma: China Fantasy Doomed on February 21, 1972 with 37th US President Richard M Nixon’s Visit to Peking.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026.
The Sanskrit word ‘guru’ translates to ‘dispeller of darkness’. Guru Purnima, marks the appearance day of Srila Vyasadeva. Guru Purnima 2026 is celebrated on Wednesday, July 29, 2026. This sacred festival honors spiritual and academic teachers, mentors, and the birth anniversary of Sage Vyasa. The Purnima Tithi began at 6:18 PM on July 28 and ends at 8:05 PM on July 29, 2026
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026.
Guru Purnima falls every year on the day of Ashadha Shukla Purnima. It is also known as Vyasa Purnima because Veda Vyasa, the sage who wrote the Mahabharata and assembled the Vedas, celebrates his birthday on this day.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026
Bharat Darshan – Bhagavan Ved Vyas – Author of Geetopanishad
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026
In the Indian tradition, Ved Vyas is the legendary author of epic poem Mahabharat, Bhagavata Purana, and several other Puranas , son of Sage Parashara, and Satyavati. He is father of Sage Shuka, King Pandu, and Minister Vidura. He is great-grandson of Maharishi Vasishta, and grandson of Sage Shakti. Ved Vyas is a historical person, a contemporary of another legendary person known as Lord Krishna whom Indians worship. As per Indian tradition, Lord Krishna belongs to a time period or “Yug” called ‘Dwapar Yug.” Apart from being a great poet, Ved Vyas is recognized as a great teacher, a spiritual guide, and a divine personality with exceptional creative writing abilities. He is often recognized as author of ‘Geetopanishad’ for the divine song, ‘Bhagavad Gita’ distills the essence of Vedic Wisdom and presents it as useful guide to live daily life experiencing peace, harmony, and tranquility.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026
In India, there was a suggestion or speculation about some unknown author, who may have inserted into epic poem Mahabharat, his/her poetical work (700 verses) that most Indians recognize as “Bhagavad Gita” and may have given credit to Ved Vyas, original author of Mahabharat. It raises issues about identity of author and the methods that people use to know the identity of any given person. In both Biology, and Medical Science, identification of individuals or individual entities is very important. Forensic Medicine deals with the identification of unknown dead bodies. In common practice, man is recognized by his occupation or actions. A poet is identified by his/her poetical composition, the literary contents of work published.
The celebration of Guru Purnima and Vyasa Purnima on Thursday, July 29, 2026
I took time to study the concepts shared in Bhagavad Gita, and Bhagavata Purana and I could easily identify the similarities of views. In Bhagavad Gita, Lord Sri Krishna spoke to Prince Arjuna. In Bhagavata Purana, in a story popularly known as ‘Prahalad Charitra’ Demon King Hiranyakashipu spoke to grieving family members following death of his brother. Both of them use the same words and share the same Vedic knowledge about life and death.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026
The poet who composed Bhagavad Gita knows concepts shared by Vedas and Upanishads. For example, we can compare ‘Parable of the Chariot’ or “Ratha Kalpana” of Katha Upanishad, Part III, verses 3 to 11 with Bhagavad Gita, Chapter III, verses 39 to 43. The author of Bhagavad Gita reconstructed Ratha Kalpana and presented his own version and there is subtle difference between those two concepts. I recognize Veda Vyas as author of Bhagavad Gita through literary analysis and by comparing views and concepts that appear in different works in different contexts. We can easily know the identity of the author by examining his work.
Comparison of Amrita Bindu Upanishad (Krishna Yajur Veda) and Bhagavad Gita:
“Eka eva hi bhutatma bhute bhute vyavasthitah ekadha bahudha caiva drsyate jala Chandravat.” (Verse # 12)
Being the One, the universal Soul is present in all beings, present in each individual living entity, and this One entity is viewed as several, different entities, just like reflection of (same) Moon seen in several pots of water.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026
The knowledge of one who sees in every living entity, though divided into innumerable forms, one undivided spiritual nature, that knowledge is to be understood as being in the mode of Goodness. Just like the verse from Amrita Bindu Upanishad, this verse speaks about one single reality pervading all existence.
Comparison of Katha Upanishad (Ratha Kalpana) and Bhagavad Gita:
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. Parable of Chariot, Ratha Kalpana of Katha Upanishad. The relationship between body, organs of sense perception, mind, seat of intellect or discernment and soul.
“atmanam rathinam viddhi, sariram ratham eva tu, buddhim tu Saradhim viddhi manah pragraham eva ca; indriyani hayan ahur visayams tesu gocaran atmendriya-mano-yuktam bhoktety ahur manisinah.” (Katha Upanishad, Part III, Sadhana, Verses 3 &4)
Know the Atman (Self) as the Master or Lord of the chariot, and the body as the chariot, know also the intellect to be the driver and mind as reins. The senses are called the horses, the sense objects are the roads; when the Atman is united with body, senses and mind, then the Wise call Him the Enjoyer.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. Body, Mind, and Soul are connected to each other, with Soul having a central controlling power over some aspects of functions of other parts or units to promote unity and harmony.
These describe hierarchy, various levels of functional control in a complex system that has different parts like body, organs of sense perception, mind, intellect, and a Master who enjoys because of functional Unity and Harmony of organizational units. In a chariot driven by horses, reins are used as a means of guiding, controlling, checking, or restraining horses. The driver uses reins to control horses to slow them down or stop or to allow them to run at full speed without restraint if required.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. The problem called Desire. There are Six kinds of Desires; 1. Kama (Lust), 2. Krodha (Anger), 3. LOBHA (Miserliness), 4. Moha (Infatuation), 5. Mada (Arrogance), and 6. Matsarya (Jealousy).
“Indriyani mano buddhir asyadhisthanam ucyate etair vimohayaty esa jnanam avrtya dehinam.” (Bhagavad Gita, Chapter III, Verse 40)
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. The problem called Desire. There are Six kinds of Desires; 1. Kama (Lust), 2. Krodha (Anger), 3. LOBHA (Miserliness), 4. Moha (Infatuation), 5. Mada (Arrogance), and 6. Matsarya (Jealousy).
It is declared that the senses, the mind, and the intelligence are the stronghold of this sensual desire (‘Kama’), covering one’s discrimination this enemy called sensual desire deludes the living entities.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. Body, Mind, and Soul are connected to each other, with Soul having a central controlling power over some aspects of functions of other parts or units to promote unity and harmony. Prince Arjuna is the Master (Soul), the Charioteer (Lord Krishna) symbolizes Buddhi (Intellect), the Reins symbolize Mind and Horses symbolize the Sense Organs, the Chariot symbolizes the human Body, and the Road represents the Pursuit to reach goal.
“tasmat tvam indriyany adau niyama bharatarsabha papmanam prajahi hy enam jnana-vijnana nasanam.”(Bhagavad Gita, Chapter III, Verse 41)
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026
Therefore O’ Arjuna, first you must bring the senses under control and directly destroy this sensual desire(‘Kama’), which is embodiment of sin and the destroyer of knowledge and self-realization.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions.
“indriyani parany ahur indriyebhyah param manah, manasas tu para buddhir yo buddheh paratas tu sah.”(Bhagavad Gita, Chapter III, Verse#42)
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions.
It is declared, the senses are superior (than insensible matter) but more than the senses, the mind is superior, but more than the mind the intelligence is superior, and more than the intelligence that which is superior is the individual consciousness (Atma).
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions.
Thus knowing the individual consciousness (Atman) to be superior to the intelligence, O’ mighty armed one, steady the mind by self-realization and conquer this insatiable enemy which presents in the form of sensual desire (Kama).
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions.
Bhagavad Gita distills wisdom of Upanishads and conveys knowledge that is of practical value and can be used as daily living guide. While Bhagavad Gita avoids analogy of chariot, the author uses the same concept to guide readers to learn The Art of Self-Discipline, a training that develops self-restraint, self-control to shape character and personal conduct that promote orderliness and efficiency in any given field of human activity or work performance.
If I have the intellectual capacity to compose 700 poems and insert them into work done by another person, I will not stop writing. I will be driven by the same creative zeal to compose more poems and keep publishing my works using my name or another name. Bhagavad Gita exposes identity of a literary genius at work, and very few people have such creative writing ability. If any of my readers have doubts about identity of Ved Vyas; you may have to support your view citing literary works of comparable merit and make claim that a different author made insertion of his/her work giving credit to Ved Vyas.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions. Ved Vyas is a historical person. Indian tradition names Time Periods as Yug and Ved Vyas belongs to Dwapara Yuga.
Bhagavad Gita refers to Kurukshetra battlefield as “Dharma Kshetra” and the concern of its author is about values, the battle between good and evil. Secondly, the conversation on the battlefield begins with Prince Duryodhana speaking to his guru Dronacharya. Here, the author is carefully suggesting that battle is not decided by relative strengths of parties engaged in war. Prince Duryodhana made an estimate of strength of Pandava Camp and was impressed by strength of Kaurava Camp. But, the author’s concern is about ‘Dharma’ or right actions and the ultimate success of right over might. Sanjaya was a disciple of author Veda Vyas and the author used his poetic imagination and freedom to confer a special ability to his student to know his thoughts as reflected in battlefield dialogue.
Hymns in praise of Maharishi Ved Vyas:
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions. Ved Vyas is a Divine Being for he shared Divine Knowledge that brings Joy, Bliss, Happiness, and Ananda.
The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions. Ved Vyas is a Divine Being for he shared Divine Knowledge that brings Joy, Bliss, Happiness, and Ananda.The celebration of Guru Purnima and Vyasa Purnima on Wednesday, July 29, 2026. To fight with an external enemy is easy. Man has to be mindful of an internal enemy called Desire which has Six Dimensions. Ved Vyas is a Divine Being for he shared Divine Knowledge that brings Joy, Bliss, Happiness, and Ananda.
Sixth-Day Adventist Holiday Tradition in Celebration of Everlasting Love
Whole Dude – Whole Coming: The Birth of Jesus is the First Singular Event; the Resurrection of Jesus and His Ascension constitutes the Second Singular Event and the Third Coming or the Future Coming, or the Final Coming constitutes the Whole Coming of Jesus for it includes a Plan for a New Heaven and Earth.
The Celebration of Everlasting Love on last Wednesday of July 2026
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love.
I am posting this article to make an announcement of the beginning of a new tradition in the national life that celebrates the central role of love in developing wholesome interpersonal human relationships.
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
Love is central to a man’s relationship to God and the man’s relations with other persons.The word Love is not mentioned in the Torah (Law) given to the Jews at Mount Sinai.
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
I conducted a study of the holiday traditions of the US and I am totally surprised to note that there is no traditional celebration of the Proclamation of the two Great Love Commandments of Jesus.
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
While retaining the essence of The Code of The Ten Words Jesus changed the Operating Principle of the Torah or The Law. Jesus instructs that the Law must be followed by His believers not through the use of force or authority but by simply embracing the equally powerful influence called Love.
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
Jesus Christ established Love as the God’s Greatest Commandment. The Gospel according to Apostle Matthew (Chapter 22, verses 37-40), andthe Gospel according to Apostle Mark (Chapter 12, verses 28-31) describe the Commandments of Love: “Love the Lord your God with all your heart and with all your soul and with all your mind and with all your strength. This is the first great commandment. The second is this: ‘Love your neighbor as yourself.’ There is no commandment greater than these. All the Law and the Prophets hang on these two Commandments.”
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting LoveSixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
The Gospel according to Apostle John, Chapter 13, verse 34 describes the need for neighborly relations among people based upon Love: “A new command I give you: Love one another, as I have loved you, so you must love one another.”
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
Whole Christ – Whole Love – Whole Gospel:
Whole Christ – Whole Love: The term “Whole Christ” refers to Jesus before His human birth, during His earthly existence, after His Resurrection, and to the Hope of His future Coming (Advent) to proclaim the ‘Kingdom of Heaven on Earth’.The term “Whole Love” describes God’s Unconditioned Love that is not determined by human knowledge and rationality. The Birth of Jesus can’t be fully accounted by human knowledge and rationality for man lacks the ability to account for his own existence.
The word Christ (Greek. Christos) refers to the Messiah whose appearance is prophesied in the Old Testament and is used as a title to describe Jesus of Nazareth. I am using the term “Whole Christ” to describe Jesus before His human birth, Jesus during the years spent on this Earth, Jesus after His Resurrection, and Jesus who gives the Hope of the Advent to proclaim The Kingdom of Heaven on Earth. The word Christ fails to communicate the entirety of Jesus and in the four Gospels we do not obtain the full picture as the event called ‘Advent’ has not yet taken place.
Whole Christ – Whole Love – Whole Law. Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
Apostle Paul in his First Epistle to Corinthians, in the New Testament Book of 1 Corinthians, Chapter 13, verses 4-8 describes the attributes of Love: “Love is patient, love is kind. It does not envy. It does not boast, it is not proud. It is not rude, it is not self-seeking, it is not easily angered, it keeps no record of wrongs. Love does not delight in evil but rejoices with the truth. It always protects, always trusts, always hopes, always perseveres. Love never fails. But where there are prophecies, they will cease; where there are tongues, they will be stilled; where there is knowledge, it will pass away.”
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
I am using the term “Whole Love” to describe God’s Unconditioned Love that is not determined or fully accounted by human knowledge and human rationality. In other words, I have no ability to empower myself to get God’s Unconditioned Love. I can’t manipulate God’s Whole Love through my actions, behavior, or even prayers. I can experience Whole Love but, I can’t explain or fully account for the existence of that Love.
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
Apostle Paul in his First Epistle to Corinthians, 1 Corinthians, Chapter 13, verse 13 shares the Spiritual Principles of Conservation: “And now these three remain: faith, hope, and love. But the greatest of these is love.”
Man exists in a world that is restless and is constantly changing. The Individual, created human being is born, grows and develops, exists with a physical identity that constantly changes under the powerful influence of Time and the event called death records the loss of that identity that is never constant at any time of its earthly existence. In the natural world, changes in appearance are governed by the Laws of Conservation like the Laws of Conservation of Mass, Energy, and Momentum. During man’s physical existence, the physical form and appearance change and yet the Spiritual Principles of Faith, Hope, and Love are conserved. Man must not depend upon his knowledge and rationality as they are always prone to change. To know the total Reality or the “WholeReality” of his ‘WholeExistence’, man needs to know the Law of Conservation of Faith, Hope, and Love.
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting Love
In the United States, we have no Law, or a cultural tradition to commemorate the event in which Jesus Christ issued the two great commandments asking people to see the Law of ‘Whole Love’ which demands, 1. The Love of God with Whole Body, Heart, Mind, and Soul, and 2. The Love of Neighbor as a need of God’s Law for man.
After my discovery of the experience of ‘Whole Love’ at Whole Foods Market, Ann Arbor, Michigan on Wednesday, July 30, 2014, I have decided to promote the establishment of a tradition’ to follow the Spirit of the ‘Whole Law’ to truly see the Commandment of Love.
To commemorate my Discovery, I am writing this appeal to ask all the members of the US Congress to approve a new Law to see the last Wednesday of July as the ‘Everlasting Love Holiday’. The choice of Wednesday is very appropriate as most other legal holidays are observed on Mondays as a matter of convenience and not for the purposes of obedience of a Divine Law which should be the source and inspiration for the Human Law. The concept of ‘Whole Love’ is the ‘Whole Law’ that is explicitly pronounced by Jesus Christ as the only Commandment that the man must follow and see in his lifetime. To acknowledge the ‘Whole Law’, to celebrate its pronouncement, we need a new tradition by instituting a new Holiday.
Sixth-Day Adventist begins a new holiday tradition on Wednesday, July 29, 2026, to celebrate Everlasting Love. I am asking all the Members of the US Congress to enact a new Law in celebration of Everlasting Love. The last Wednesday of July should be a legal holiday to celebrate God’s Everlasting LoveWhole Dude – Whole Coming: The Birth of Jesus is the First Singular Event; the Resurrection of Jesus and His Ascension constitutes the Second Singular Event and the Third Coming or the Future Coming, or the Final Coming constitutes the Whole Coming of Jesus for it includes a Plan for a New Heaven and Earth.Whole Dude – Whole Coming: The Birth of Jesus is the First Singular Event; the Resurrection of Jesus and His Ascension constitutes the Second Singular Event and the Third Coming or the Future Coming, or the Final Coming constitutes the Whole Coming of Jesus for it includes a Plan for a New Heaven and Earth.
The Celebration of Love demands a new Holiday Tradition called Christmas in July.
The Celebration of Love demands a new Holiday Tradition called Christmas in July.
On Last Wednesday, 29th Day of July 2026, Whole Dude celebrates the Whole Cookie Day to declare, “I am the Creme of Life. The Vanilla Cookie gives me the feeling that I am the most Loved Person in the World. And the Chocolate Cookie gives me the feeling that I have never, ever experienced for being so much in Love during my entire Life.” For I am the Creme of Life, I can experience all the dimensions of Whole Love at the same time.
Whole Dude – Whole Love – Whole Discovery: The 3-dimensional Love can be stated as, 1. Love of God, 2. Self-Love, and 3. Love of another person.
I will be shouting “Shavuot”, “Shavuot”, and “Shavuot” until we start a new Holiday Tradition to celebrate the proclamation of the two Great Commandments that replaced the ‘Torah’ to all people who are waiting for fulfillment in the Kingdom of God. The idea is that of promoting the recognition of Love as a Natural Law that brings Unity and synchronizes all other faiths and beliefs by a single Universal Principle.
Whole Team Members who like to join the Whole Celebration can apply for the same by Leaving a Comment on this blog post. Please scroll down to find the Leave a Comment tab. Please click on it and fill in your comment in the box. Your private information and full name need not be disclosed. Your e-mail ID will not be published.
Whole Dude – Whole Creme – Whole Celebration: The Celebration of Love demands a new Holiday Tradition called Christmas in July. In Jewish tradition, the day of proclamation of Torah at Mount Sinai is celebrated as Shavout. Among Christians of all denominations there is no comparable holiday tradition to celebrate the proclamation of the two Great Love Commandments of Jesus Christ.
The word Love does not appear in the Torah ( Law) given to the Jews at Mount Sinai. I conducted a study of the holiday traditions of the US and I am totally surprised to note that there is no traditional celebration of the Proclamation of the two Great Love Commandments of Jesus Christ. The Jewish Holiday “Shavuot” celebrates the giving of the Torah (the Law or Instruction) to the Jews. God gave the Ten Commandments (The Decalogue, The Code of The Ten Words)on the sixth night of the Hebrew month of ‘Sivan’. Shavuot always falls 50 days (Pentecost) after the second night of Passover. The 49 days between Passover and Shavuot are known as ‘Omer’. Jesus Christ retains the essence of The Code of The Ten Words; but, changed the Operating Principle of the Torah or The Law. Jesus instructs that the Law would be followed by His believers not through the use of force or authority but by simply embracing the equally powerful influence called “Love.”
Whole Dude – Whole Creme – Whole Celebration: The Celebration of Love demands a new Holiday Tradition called Christmas in July.
I am posting this article to make an open appeal to all the members of the US Congress to pass a decree or law to commence a new tradition in the national life that celebrates the central role of love in developing wholesome human relationships. I am using the term ‘Whole Self’ to describe the perfect unity of body, mind, heart, soul, and God that establishes man as a Whole Being. Love is central to man’s relationship to God and man’s relations with other persons. The term love includes the feelings or the emotion of love expressed by a person (The Subject) and it involves a personal experience evoked when another person (The Object) reflects the feelings of love. Love has to be known as The Medium that generates the attachment or devotion to another person; and this attachment implies connection by ties of affection, sexual attraction, devotion, friendship, goodwill, compassion, respect, trust, and commitment. This kind of care and concern for a person, or persons in a relationship could be called ‘Whole Love’ if whatever is done for Love occurs beyond good and evil.
Whole Dude – Whole Creme – Whole Celebration: The Celebration of Love demands a new Holiday Tradition called Christmas in July.
The concept of Holiday begins with the story of creation as revealed in the Book of Genesis and it involves the observance of a ‘Holy Day’. “And God blessed the seventh day and made it holy, because on it He rested from all the work of creating that He had done (Genesis, Chapter 2, verse#3).”
Whole Dude – Whole Creme – Whole Celebration: The Celebration of Love demands a new Holiday Tradition called Christmas in July.
Holiday is a day of freedom from labor sanctioned by God, and it is set aside for leisure and recreation to renew man’s relationship with his Creator. In Civil Society, certain days are set aside by Law or Custom and Traditions for the suspension of official business activities and very often in commemoration of some important events in national life. I am using the term ‘Whole Holiday’ to recognize a specific day that is set aside by Human Law in recognition of the Divine Law that is conducive to the development of harmonious, or wholesome interpersonal relationships that are essential to promote the health, and well-being of all people. In the US, there are several holidays that are legal and none of them directly address the central issue of developing Love relationships.
Whole Dude – Whole Creme – Whole Celebration: The Celebration of Love demands a new Holiday Tradition called Christmas in July.
Christmas Day Holiday celebration reflects the very essence of Christianity. The Gospel according to Apostle John, Chapter 3, verse# 16 declares: “For God so loved the world that He gave His only begotten Son, that whoever believes in Him shall not perish but have eternal life.” The Christmas tradition is about the Joy associated with the birth of baby Jesus and the exchange of gifts to express the sense of happiness. Christmas holiday is not in the remembrance of God’s Law. Jesus Christ established Love as the God’s Greatest Commandment. The Gospel according to Apostle Matthew (Chapter 22, verses#37-40), and The Gospel according to Apostle Mark (Chapter 12, verses# 28-31) describe the Commandments of Love: “Love the LORD your God with all your heart and with all your soul and with all your mind and with all your strength. This is the first great commandment. The second is this: ‘Love your neighbor as yourself.’ There is no commandment greater than these. All the Law and the Prophets hang on these two Commandments.” The Gospel according to Apostle John, Chapter 13, verse# 34 describes the need for neighborly relations among people based upon Love: “A new command I give you: Love one another, as I have loved you, so you must love one another.”
Whole Love – Whole Tradition – Whole Law – Whole Holiday:
“I am the Creme of Life. The Vanilla Cookie gives me the feeling that I am the most Loved Person in the World. And the Chocolate Cookie gives me the feeling that I have never, ever experienced for being so much in Love during my entire Life.” I discovered the three fundamental dimensions of Love, which have to come together to give the experience of Whole Love.
In the United States, we have no Law, or a cultural tradition to commemorate the event in which Jesus Christ issued the two great commandments asking people to observe the Law of ‘Whole Love’ which demands, 1. The Love of God with Whole Body, Heart, Mind, and Soul, and 2. The Love of Neighbor as a requirement of God’s Law for man. After my ‘Whole Discovery’, the discovery of the experience of ‘Whole Love’ on Wednesday, July 30, 2014, I have decided to promote the establishment of a ‘Whole Tradition’ to follow the Spirit of the ‘Whole Law’ to truly observe the Commandment of ‘Whole Love’. To commemorate my ‘Whole Discovery’, I am writing this appeal to ask all the members of the US Congress to approve a new Law to observe the last Wednesday of July as the ‘Whole Love Holiday’. The choice of Wednesday is very appropriate as most other legal holidays are observed on Mondays as a matter of convenience and not for the purposes of obedience to a Divine Law which should be the source and inspiration for the Human Law. The concept of ‘Whole Love’ represents the ‘Whole Law’ that is explicitly pronounced by Jesus Christ as the only Commandment that man must follow and observe in his lifetime. To acknowledge the ‘Whole Law’, to celebrate its pronouncement, we need a new ‘Whole Tradition’ which is reflected by instituting a new ‘Whole Holiday’.
Whole Love – Whole Holiday – Christmas in July:
Whole Dude – Whole Creme – Whole Celebration: The Celebration of Love demands a new Holiday Tradition called Christmas in July.
The term ‘Cookie’ is used to describe a small sweet cake usually flat and often crisp. The word ‘Cookie’ may also be used to describe an attractive, young woman. As Sigmund Freud had explained, all kinds of love have an element of sexual attraction and it is inherently natural as such attraction is the fundamental nature of all living things that are governed by the Natural Law of Generation and Propagation. So, I love my ‘Cookies’ even if it may imply the Love of more than one person. The ‘Whole Law’ mandates the Love of more than one person.
Whole Dude – Whole Creme – Whole Celebration: The Celebration of Love demands a new Holiday Tradition called Christmas in July.
The Vanilla Cookie symbolizes God’s Unconditioned Love for the man and the Chocolate Cookie symbolizes the man’s love of his neighbor. The Vanilla Cookie always assures me and comforts me for I exist as an Object that is always loved. That makes it easier for me to exist as the Subject who unfailingly loves the neighbor. The Commandment or the Divine Law that demands people to ‘Love thy Neighbor’ must be celebrated in a tradition similar to the Jewish Holiday that celebrates the Proclamation of The Ten Commandments. In my opinion, it is not about imposition of religion by State. The State has declared its Independence on July 04, 1776 claiming Natural Rights and quoted the Principles of Natural Law to justify its demand for Independence from the British Crown. Further, the Supreme Law of the US is the Constitution of the US and it gives the Right to Life and supports the Pursuit of Happiness. The opposite of Love is called ‘Hate’ and it precisely undermines the citizens’ right to life and to the pursuit of happiness. The remembrance of the ‘Love Commandments’, the honoring of its Proclamation and a traditional celebration of ‘Whole Love’ will definitely promote the development of social harmony, is conducive to peaceful enjoyment of life and will establish tranquility in human interactions. We need Wholesome Relations between individuals and between nations to prepare the Whole World for the Second Coming of the Christ.
Each one of the first 200 Whole Team Members who apply to join the Whole Celebration will get a 20 Oz box of 365 Everyday Value Mismatched Sandwich Cremes as Sign-Up Bonus (Milk not included). Please scroll down to find the tab ‘Leave a Comment’.
“I am the Creme of Life. The Vanilla Cookie gives me the feeling that I am the most Loved Person in the World. And the Chocolate Cookie gives me the feeling that I have never, ever experienced for being so much in Love during my entire Life.” I discovered the three fundamental dimensions of Love, which have to come together to give the experience of Whole Love.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign DayWhole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign DayWhole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
Yes indeed. Life is Complicated. What is this Day in History? The complexity of Life is about finding the Connection between the Date and Life. Man’s Plan for Life must come together with God’s Purpose in Life to win the Battle Against Spiritual Wickedness.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
July 26, This Day in my Life:
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign DayWhole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign DayWhole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
Sunday, 26th Day of July 2026. I am dedicating this Day of my life to the Anti-Slavery Campaign, Repeal PRWORA Project, and The Great Awakening Movement claiming that I will not wrestle or struggle against people but, I will confront spiritual wickedness in the highest places.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
On the 26th Day of July 1970, I started my preparation to participate in the CIA’s Secret War in Occupied Tibet. In man’s plan, I exist as a mere pawn used in the War on Communism, the legacy of the Cold War Era of Geopolitics. What is God’s Plan for my life?
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
On Sunday, 26th Day of July 2026, I confess that I have not yet arrived at the final destination of my life. I continue to struggle for my personal freedom and I continue to wrestle against the dark forces keeping Tibetans away from freedom.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude celebrates the CIA Connection on Sunday, July 26, 2026. Dr. Sarvepalli Radhakrishnan and the history of Special Frontier Force-Establishment No. 22, Vikas Regiment: In India, school children celebrate Dr. Radhakrishnan’s birthday (05 September) as Teacher’s Day and every year that I spent as a student, I had a special reason to remember my family connection with his daughter.
On this day, July 26, 1947, President Harry Truman signed the National Security Act that set up the Central Intelligence Agency. The Cold War Era secret diplomacy shaped the course of my life that began in Mylapore, Madras, Chennai. My Life’s Journey from Mylapore to Chakrata, and later to Ann Arbor, Michigan is a direct consequence of my CIA Connection predestined on July 26, 1970.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
I was granted Short Service Regular Commission in the Indian Army Medical Corps in the rank of Lieutenant on July 26, 1970. On completion of my military training, I received the promotion, the substantive rank of Captain with effect from July 26, 1971. My first posting of Military Service sent me to Special Frontier Force, Headquarters Establishment No. 22, Vikas Regiment in support of CIA’s Mission in South Asia. I describe “My CIA Connection” as ‘Kasturi-Sarvepalli-Mylapore-Madras-India-Tibet-US Connection’.
I was granted President’s Commission to serve in the Regular Army and was appointed in the Rank of Lieutenant on 26 July, 1970.Doomed Gun of Doom Dooma: China Fantasy Doomed on February 21, 1972 with 37th US President Richard M Nixon’s Visit to Peking.Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
On Saturday, July 26, 1986, I left Muscat, Oman to arrive in the United States in search of the Final Destination of my Life.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
On Sunday, July 26, 2026, I live in Ann Arbor, Michigan still hoping to arrive at the Final Destination of my Life. My CIA Connection may either sanction Slavery in the United States or that of a Prisoner of War (POW) in the Enemy’s Camp.
Man’s Plan for July 26 vs God’s Plan for July 26. July 26th, 2026. This day of my life. My CIA connection was made possible because of the Cold War Era secret diplomacy to wage War on Communism.
This Day in My Life – July 26 – My CIA Connection. God’s Calendar predestined meeting between Indian Prime Minister Jawaharlal Nehru and the US President Harry Truman. Cold War History. War on Communism.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
President Harry S. Truman signs the National Security Act, which becomes one of the most important pieces of Cold War legislation. The act established much of the bureaucratic framework for foreign policymaking for the next 40-plus years of the Cold War.
By July 1947, the Cold War was in full swing. The United States and the Soviet Union, once allies during World War II, now faced off as ideological enemies. In the preceding months, the administration of President Truman had argued for, and secured, military and economic aid to Greece and Turkey to assist in their struggles against communist insurgents. In addition, the Marshall Plan, which called for billions of dollars in U.S. aid to help rebuild war-torn Western Europe and strengthen it against possible communist aggression, had also taken shape. As the magnitude of the Cold War increased, however, so too did the need for a more efficient and manageable foreign policymaking bureaucracy in the United States. The National Security Act was the solution.
The National Security Act had three main parts. First, it streamlined and unified the nation’s military establishment by bringing together the Navy Department and War Department under a new Department of Defense. This department would facilitate control and utilization of the nation’s growing military. Second, the act established the National Security Council (NSC). Based in the White House, the NSC was supposed to serve as a coordinating agency, sifting through the increasing flow of diplomatic and intelligence information in order to provide the president with brief but detailed reports. Finally, the act set up the Central Intelligence Agency (CIA). The CIA replaced the Central Intelligence Group, which had been established in 1946 to coordinate the intelligence-gathering activities of the various military branches and the Department of State. The CIA, however, was to be much more–it was a separate agency, designed not only to gather intelligence but also to carry out covert operations in foreign nations.
The National Security Act formally took effect on September 1947. Since that time, the Department of Defense, NSC, and CIA have grown steadily in terms of size, budgets, and power. The Department of Defense, housed in the Pentagon, controls a budget that many Third World nations would envy. The NSC rapidly became not simply an information organizing agency, but one that was active in the formation of foreign policy. The CIA also grew in power over the course of the Cold War, becoming involved in numerous covert operations. Most notable of these was the failed Bay of Pigs operation of 1961, in which Cuban refugees, trained and armed by the CIA, were unleashed against the communist regime of Fidel Castro. The mission was a disaster, with most of the attackers either killed or captured in a short time. Though it had both successes and failures, the National Security Act indicated just how seriously the U.S. government took the Cold War threat.
Man’s Plan for July 26 vs God’s Plan for July 26. July 26th, 2026. This day of my life. My CIA connection is made possible by President Harry Truman’s War on Communism.
This Day in My Life – July 26 – My CIA Connection. God’s Calendar predestined events of my Life’s Journey From Mylapore, Madras to Ann Arbor, Michigan. Thanks to US President Harry S. Truman’s War on Communism.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
This Day in My Life – July 26 – My CIA Connection. Cold War Era History. God’s Calendar predestined events of My Life’s Journey From Mylapore, Madras to Ann Arbor, Michigan. Thanks to US President Harry S. Truman’s War on Communism.
Man’s Plan for July 26 vs God’s Plan for July 26. July 26th, 2026. This day of my life. My CIA connection promises to impose either slavery in the US or that of a Prisoner of War (POW) in the Enemy’s camp. Man’s plan vs God’s plan will decide the ultimate outcome.
This Day in My Life – July 26 – My CIA Connection. In Man’s Plan, I exist as a mere Pawn used in War on Communism, Legacy of Cold War Era Geopolitics.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
The celebration of the CIA Connection on Sunday, July 26, 2026. What is God’s Plan?
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign DayWhole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
Commemoration of the National Security Act of 1947 – July 26, 2026 marked as Anti-Slavery Campaign Day
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
On this Day, July 26, 1947, President Harry Truman signed The National Security Act that set up The Central Intelligence Agency that plays a crucial role in promoting US Policy in support of Freedom, Democracy, Peace and Human Rights.
Whole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign DayWhole Warfare: The Commemoration of the National Security Act of 1947. Whole Dude observes July 26, 2026 as Anti-Slavery Campaign Day
Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.
All said and done, the Kargil War stands out as the proud symbol of Indian Identity and Indian Unity while confronting an adverse situation imposed by the evil, unfair, and unjust actions of India’s Enemy.
26th July is an important date in my memory for I joined the Indian Army Medical Corps at Officers Training School, Army Medical Corps Centre at Lucknow on this date in 1970.
Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.
The Bofors 155mm howitzers played a remarkable role in the Kargil War. I know the Indian Army Chief who purchased the Bofors Guns that played a major role in the Kargil War of 1999. General Krishnaswamy Sundarji, PVSM (28 April 1928 – 8 February 1999), was the Chief of Army Staff of the Indian Army from 1986 to 1988. He was the last former British Indian Army officer to command the Indian Army. I served under his Command when he was the General Officer-Commanding-in-Chief of the First Armoured Division between 1976-78.
I commemorate the Victory in Kargil War of 1999 to acknowledge the fact of Special Frontier Force’s participation in this herculean war effort.
Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas. Every year, the Indian Army soldiers prepare to celebrate Kargil Vijay Diwas (Victory day) celebrations at the war memorial in DrassWhole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.
Kargil Vijay Diwas: The 26th Anniversary of Kargil Vijay Diwas will be celebrated across the country on Sunday, July 26, 2026. The Indian armed forces defeated attempts by Pakistan to capture strategic heights in Kargil in 1999. The military action to evict the enemy occupier was named ‘Operation Vijay’. It was on July 26, 1999, Indian Army had declared successful culmination of ‘Operation Vijay’, declaring a victory after nearly three-month-long battles against Pakistan on the icy heights of Kargil. India had lost 527 soldiers in the war.
Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas. General VP Malik, Indian Army Chief, during Kargil conflict. (Express Archive Photo)
The nation is remembering its war heroes and paying tributes to Martyrs on Kargil Vijay Diwas. As many as 527 soldiers from the Indian Armed Forces lost their lives during the war. The Kargil Vijay Diwas not only embarks upon India’s win but also pays homage to the fallen heroes who fought valiantly for the nation, and sacrificed their lives to make ‘Operation Vijay’ a success.
The occasion commemorates the glorious victory of the Indian armed forces against the Pakistan Army intruders in the Kargil, Drass and Batalik sectors in 1999.
Battle of Tiger Hill, Drass Sector, July 02-04, 1999. Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Kargil 2021: Chief of Defence Staff General Bipin Rawat visits Dras Sector along the Line of Control (LOC)Indian Army soldiers during a special event narrating the stories of Operation VIJAY at Lamochen near Dras in Ladakh, Sunday, July 25, 2021. (PTI)The Indian Air Force code named its Operation as Op Safed Sagar (Operation White Sea).The Indian Air Force code named its Operation as Op Safed Sagar (Operation White Sea).Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.The Indian Air Force code named its Operation as Op Safed Sagar (Operation White Sea).Friday, July 26, 2024. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 25th Anniversary of Kargil Vijay Diwas. The Indian Air Force code named its Operation as Op Safed Sagar (Operation White Sea).Friday, July 26, 2024. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 25th Anniversary of Kargil Vijay Diwas. The Indian Air Force code named its Operation as Op Safed Sagar (Operation White Sea).Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas. Special Frontier Force trains at Sarsawa Air Base.The Kargil War Memorial at the foothill of Tololing hill, where Indian troops fought one of the toughest battles of the Kargil war. The memorial has the tombstones of the martyrs and a museum.The Kargil War Memorial at the foothill of Tololing hill, where Indian troops fought one of the toughest battles of the Kargil war. The memorial has the tombstones of the martyrs and a museum.The Kargil War Memorial at the foothill of Tololing hill, where Indian troops fought one of the toughest battles of the Kargil war. The memorial has the tombstones of the martyrs and a museum.Indian soldiers on a mountain peak during the war. The Pakistan army had captured nearly 100 km of Indian territory inside the Line of Control. Indian soldiers paid in their blood to regain the land. Photograph: Rediff.comThe Indian Prime Minister Atal Bihari Vajpayee along with the Defence Minister George Fernandes, crouching, third from left, the Jammu and Kashmir Governor Girish Chandra ‘Gary’ Saxena, standing second from left, and the Indian Army Chief General Ved Prakash Malik, fourth from right, meet the troops in Kargil. Photograph: Rediff.comParam Vir Chakra awardees Rifleman Sanjay Kumar, left, and Grenadier Yoginder Yadav, center, with Mahavir Chakra awardee Lieutenant (now Colonel) Balwan Singh, right. Grenadier Yadav and Lieutenant Balwan Singh were in the commando platoon that led the final assault on Tiger Hill. Their bravery that night is the stuff of legend. Photograph: Rediff.com.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Captain Vikram Batra in the Drass sector.Special Frontier Force pays tribute to Kargil War Hero, Captain Vikram Batra, 13 Jammu and Kashmir Rifles, who made the supreme sacrifice on July 07, 1999.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Special Frontier Force pays tribute to Kargil War Hero, Captain Keishing Clifford Nongrum, 12 JAK LI, who made the supreme sacrifice on July 01, 1999Special Frontier Force pays tribute to Kargil War Heroes of the Naga Regiment who made the supreme sacrifice on July 06-07, 1999.Special Frontier Force pays tribute to Kargil War Hero,Subedar Nirmal Singh, VrC, 8 SIKH who made the supreme sacrifice on July 05, 1999.Special Frontier Force pays tribute to Kargil War Hero, Captain Jerry Prem Raj, 158 Medium Regiment (Artillery) who made the supreme sacrifice on July 07, 1999.Special Frontier Force pays tribute to Kargil War Hero, Lieutenant Deepankar Kapoor Singh Sharawat, 2 NAGA for his gallant action on July 08, 1999.Special Frontier Force pays tribute to Kargil War Hero, Captain Amit Velma, 9 MAHAR, who made the supreme sacrifice on July 04, 1999.Special Frontier Force pays tribute to Kargil War Hero, Naik V.N. Radha Kumar, 9 Para SF who made the supreme sacrifice on July 01, 1999.Special Frontier Force pays tribute to Kargil War Hero, Sepoy Narendra Singh Jakhar, 8 JAT who made the supreme sacrifice on July 09, 1999.CQMH Amruddin, 22 Grenadiers made the supreme sacrifice on July 03, 1999.Havildar Sis Ram Gill, Vir Chakra, 8 JAT made the supreme sacrifice on July 09, 1999.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.The Bofors 155mm howitzers played a remarkable role in the Kargil War. Photograph: Fayaz Kabli/ReutersIndian soldiers show the victory sign in Drass after India captured Tiger Hill on July 4, 1999. Photograph: Kamal Kishore/ReutersWhole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.Naik Digendra Kumar served the 2nd Battalion of the Rajputana Rifles during the 1999, Kargil War before retiring in 31st July, 2005. He was awarded the Mahavir Chakra on 15th August 1999, for his heroism in the battlefield.Major Vivek Gupta of the 2nd Battalion, Rajputana Rifles, died in the Kargil conflict on June 12, 1999, after capturing two important posts in the Drass sector. He was felicitated with Maha Vir Chakra for his heroism at the war front.July 26, 2024. Special Frontier Force commemorates the Victory in Kargil War of 1999. Colonel Sonam Wangchuk is an Indian Army officer serving the Ladakh scouts regiment. In the 1999 Kargil War, then Major Wangchuk led an operation against Pakistani troops on Chorbat La Top, for which he was awarded the Maha Vir Chakra.Major Rajesh Singh Adhikari was an Indian Army Officer who died in the Battle of Tololing on May 30, 1999 during the Kargil War. He was awarded the gallantry honor, Maha Vir Chakra for his bravery in warfare.Indian Army Major Padmapani Acharya of the 2nd Battalion, Rajputana Rifles, was killed by the enemy at Lone Hill on June 28, 1999, during the Kargil conflict. He was awarded the Maha Vir Chakra for his heroic act of bravery despite succumbing to injuries.Lieutenant Keishing Clifford Nongrum of the 12th Battalion, Jammu and Kashmir Light Infantry, attained martyrdom on July 1st, 1999 while capturing Point 4812 during the Kargil War. He was honored with Maha Vir Chakra for his chivalry in the combat operations.Captain Anuj Nayyar was an Indian Army officer of the 17th Battalion, Jat Regiment, who laid down his life while battling at the Tiger Hill on 7th July 1999 during the Kargil War. He was posthumously awarded the Maha Vir Chakra for his exemplary valor during combat operations.The Victorious Indian Army Jawans of 18 Grenadiers after recapturing the Tiger Hill in Drass sector of Jammu and Kashmir. (Express archive)Whole Victory – Sunday, July 26, 2026. Special Frontier Force commemorates the Victory in Kargil War of 1999. The 27th Anniversary of Kargil Vijay Diwas.
Whole Dude – Whole Warfare: Commemoration of the National Security Act of 1947. Whole Dude at Whole Foods observes July 26, 2026 as Anti-Slavery Campaign Day
Yes indeed. Life is Complicated. What is this Day in History? The complexity of Life is about finding the Connection between the Date and Life. Man’s Plan for Life must come together with God’s Purpose in Life to win the Battle Against Spiritual Wickedness.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
July 26, This Day in my Life:
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
Sunday, 26th Day of July 2026. I am dedicating this Day of my life to the Anti-Slavery Campaign, Repeal PRWORA Project, and The Great Awakening Movement claiming that I will not wrestle or struggle against people but, I will confront spiritual wickedness in the highest places.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
On the 26th Day of July 1970, I started my preparation to participate in the CIA’s Secret War in Occupied Tibet. In man’s plan, I exist as a mere pawn used in the War on Communism, the legacy of the Cold War Era of Geopolitics. What is God’s Plan for my life?
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
On Sunday, 26th Day of July 2026, I confess that I have not arrived at the final destination of my life. I continue to struggle for my personal freedom and I continue to wrestle against the dark forces keeping Tibetans away from freedom.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026. Dr. Sarvepalli Radhakrishnan and the history of Special Frontier Force-Establishment No. 22, Vikas Regiment: In India, school children celebrate Dr. Radhakrishnan’s birthday (05 September) as Teacher’s Day and every year that I spent as a student, I had a special reason to remember my family connection with his daughter.
On this day, July 26, 1947, President Harry Truman signed the National Security Act that set up the Central Intelligence Agency. The Cold War Era secret diplomacy shaped the course of my life that began in Mylapore, Madras, Chennai. My Life’s Journey from Mylapore to Chakrata, and later to Ann Arbor, Michigan is a direct consequence of my CIA Connection destined on July 26, 1970.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026I was granted President’s Commission to serve in the Regular Army and was appointed in the Rank of Lieutenant on 26 July, 1970.
I was granted Short Service Regular Commission in the Indian Army Medical Corps in the rank of Lieutenant on July 26, 1970. On completion of my military training, I received the promotion, the substantive rank of Captain with effect from July 26, 1971. My first posting of Military Service sent me to Special Frontier Force, Headquarters Establishment No. 22, Vikas Regiment in support of CIA’s Mission in South Asia. I describe “My CIA Connection” as ‘Kasturi-Sarvepalli-Mylapore-Madras-India-Tibet-US Connection’.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
On July 26, 1986, I left Muscat, Oman to arrive in the United States in search of the Final Destination of my Life.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
On Sunday, July 26, 2026, I live in Ann Arbor, Michigan still hoping to arrive at the Final Destination of my Life. My CIA Connection may either sanction Slavery in the United States or that of a Prisoner of War (POW) in the Enemy’s Camp.
Man’s Plan for July 26 vs God’s Plan for July 26. July 26th, 2026. This day of my life. My CIA connection was made possible because of the Cold War Era secret diplomacy to wage War on Communism.
This Day in My Life – July 26 – My CIA Connection. God’s Calendar predestined meeting between Indian Prime Minister Jawaharlal Nehru and the US President Harry Truman. Cold War History. War on Communism.
Man’s Plan for July 26 vs God’s Plan for July 26. The Rudi Connection at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
President Harry S. Truman signs the National Security Act, which becomes one of the most important pieces of Cold War legislation. The act established much of the bureaucratic framework for foreign policymaking for the next 40-plus years of the Cold War.
By July 1947, the Cold War was in full swing. The United States and the Soviet Union, once allies during World War II, now faced off as ideological enemies. In the preceding months, the administration of President Truman had argued for, and secured, military and economic aid to Greece and Turkey to assist in their struggles against communist insurgents. In addition, the Marshall Plan, which called for billions of dollars in U.S. aid to help rebuild war-torn Western Europe and strengthen it against possible communist aggression, had also taken shape. As the magnitude of the Cold War increased, however, so too did the need for a more efficient and manageable foreign policymaking bureaucracy in the United States. The National Security Act was the solution.
The National Security Act had three main parts. First, it streamlined and unified the nation’s military establishment by bringing together the Navy Department and War Department under a new Department of Defense. This department would facilitate control and utilization of the nation’s growing military. Second, the act established the National Security Council (NSC). Based in the White House, the NSC was supposed to serve as a coordinating agency, sifting through the increasing flow of diplomatic and intelligence information in order to provide the president with brief but detailed reports. Finally, the act set up the Central Intelligence Agency (CIA). The CIA replaced the Central Intelligence Group, which had been established in 1946 to coordinate the intelligence-gathering activities of the various military branches and the Department of State. The CIA, however, was to be much more–it was a separate agency, designed not only to gather intelligence but also to carry out covert operations in foreign nations.
The National Security Act formally took effect on September 1947. Since that time, the Department of Defense, NSC, and CIA have grown steadily in terms of size, budgets, and power. The Department of Defense, housed in the Pentagon, controls a budget that many Third World nations would envy. The NSC rapidly became not simply an information organizing agency, but one that was active in the formation of foreign policy. The CIA also grew in power over the course of the Cold War, becoming involved in numerous covert operations. Most notable of these was the failed Bay of Pigs operation of 1961, in which Cuban refugees, trained and armed by the CIA, were unleashed against the communist regime of Fidel Castro. The mission was a disaster, with most of the attackers either killed or captured in a short time. Though it had both successes and failures, the National Security Act indicated just how seriously the U.S. government took the Cold War threat.
Man’s Plan for July 26 vs God’s Plan for July 26. July 26th, 2026. This day of my life. My CIA connection is made possible by President Harry Truman’s War on Communism.
This Day in My Life – July 26 – My CIA Connection. God’s Calendar predestined events of my Life’s Journey From Mylapore, Madras to Ann Arbor, Michigan. Thanks to US President Harry S. Truman’s War on Communism.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
This Day in My Life – July 26 – My CIA Connection. Cold War Era History. God’s Calendar predestined events of My Life’s Journey From Mylapore, Madras to Ann Arbor, Michigan. Thanks to US President Harry S. Truman’s War on Communism.
Man’s Plan for July 26 vs God’s Plan for July 26. July 26th, 2026. This day of my life. My CIA connection promises to impose either slavery in the US or that of a Prisoner of War (POW) in the Enemy’s camp. Man’s plan vs God’s plan will decide the ultimate outcome.
This Day in My Life – July 26 – My CIA Connection. In Man’s Plan, I exist as a mere Pawn used in War on Communism, Legacy of Cold War Era Geopolitics.
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026. What is God’s Plan?
Man’s Plan for July 26 vs God’s Plan for July 26. Whole Dude at Whole Foods celebrates the CIA Connection on Sunday, July 26, 2026
Commemoration of the National Security Act of 1947 – July 26, 2026 marked as Anti-Slavery Campaign Day
Whole Dude – Whole Warfare: Commemoration of The National Security Act of 1947. July 26, 2026, marked as Anti-Slavery Campaign Day.
On this Day, July 26, 1947, President Harry Truman signed The National Security Act that set up The Central Intelligence Agency that plays a crucial role in promoting US Policy in support of Freedom, Democracy, Peace and Human Rights.
Whole Dude – Whole Warfare: Commemoration of The National Security Act of 1947. July 26, 2026, marked as Anti-Slavery Campaign Day.Whole Dude – Whole Warfare: Commemoration of The National Security Act of 1947. July 26, 2026, marked as Anti-Slavery Campaign Day.
Whole Legacy – The US Policy on Tibet is not Working
US Policy on Tibet is not working. It will not work until and unless the US revises US Policy on Communist China. If Communism remains the ruling doctrine of China, no US Policy on Tibet will work. United States has no choice other than that of containing, engaging, confronting, and opposing China’s Communism.US President Donald Trump (2nd L) holds a bilateral meeting with China’s President Xi Jinping (R) at Trump’s Mar-a-Lago estate in Palm Beach, Florida, US, on April 7, 2017. Photo: Reuters
US Policy on Tibet is not working. It will not work until and unless the US revises US Policy on Communist China. If Communism remains the ruling doctrine of China, no US Policy on Tibet will work. United States has no choice other than that of containing, engaging, confronting, and opposing China’s Communism.
Rudra Narasimham Rebbapragada
Special Frontier Force-Establishment 22-Vikas Regiment
DOOMED AMERICAN CHINA FANTASY. US CONGRESSMAN JIM McGOVERN, D-Mass., CALLS FOR NEW US POLICY ON TIBET.
FILE – Rep. Jim McGovern, D-Mass., speaks on Capitol Hill in Washington, May 7, 2014. McGovern is calling for a new U.S. policy on Tibet.
WASHINGTON —
Congressman Jim McGovern is calling for a new U.S. policy on Tibet, saying “the status quo isn’t working” and urging U.S. businesses to raise the issue of human rights in Tibet with Chinese business partners.
“It’s important that the U.S. have a policy toward Tibet because the status quo isn’t working,” McGovern, a Democrat from Massachusetts, told VOA Mandarin. “The Chinese government is just getting worse on a whole range of issues — jailing more and more Tibetans in Tibet and in the Tibetan region, so I think we need to re-assess. … We need to start walking the walk.”
US Congressman Calls for New US Policy on Tibet
China says the Himalayan region has been part of its realm for more than seven centuries and considers the Dalai Lama, the Tibetan spiritual leader, to be a dangerous separatist.
Many Tibetans insist they were essentially independent for most of that time and have protested what they regard as China’s heavy-handed rule since Chinese army units crossed the Yangtze River into eastern Tibet in 1950.
Congressional visit
Last month, McGovern traveled to Nepal and the north Indian hill town of Dharamsala, where the Dalai Lama has been in exile from Tibet for almost 60 years. The eight-person House delegation led by Rep. Nancy Pelosi, a Democrat from California, wanted to make China aware that they would not stand down in their campaign for human rights in Tibet.
Watch: US Congressman Calls for China to Show Flexibility on Tibet
The delegation, including a lone Republican, Wisconsin’s Jim Sensenbrenner, met with the Dalai Lama.
“His Holiness is not a separatist … but he wants to go home and so do his people,” McGovern said.
“China is one of the great powers of the world, they’re doing great things on climate change,” he said, adding he’s always puzzled that China “is paranoid over this monk, and paranoid over his message.”
McGovern is the sponsor of the Reciprocal Access to Tibet Act of 2017. He introduced the bipartisan bill in the House in April with Congressman Randy Hultgren, a Republican from Illinois. Marco Rubio, a Republican from Florida, and Tammy Baldwin, a Democrat from Wisconsin, introduced a companion bill in the Senate.
US Congressman Poses Reciprocal Access to Tibet Act
Travel in US
McGovern described his bill as saying, “we will treat you like you treat us” in that it calls for restricting where Chinese can visit in the United States in the same way China restricts United States officials, journalists and other citizens in Tibetan areas of the People’s Republic of China.
“If China wants its citizens and officials to travel freely in the U.S., Americans must be able to travel freely in China, including Tibet,” McGovern echoes on his website.
He also wants the U.S. to “publicly call on the Chinese government to restart the direct dialog that used to exist between the Chinese government and the Tibetan people. That needs to be restarted.”
McGovern said he wants the United States to appoint a special coordinator on Tibet as soon as possible to help elevate these issues.
“We’ve also talked about working with other countries and establishing what we call A Group of Friends on Tibet who would meet regularly and publicly to assess the situation in Tibet, and whether there’s been progress or not,” he added.
US Congressman: US Firms Can Raise Issue of Tibet With Chinese Counterparts
McGovern, who is co-chair of the bipartisan Tom Lantos Human Rights Commission, told VOA that while U.S. and Chinese companies profit from trading with each other, if U.S. companies “know what’s happening and you don’t say anything [about human rights in Tibet], then you’re complicit. China wants to do business with you. You want to do business with China but that doesn’t mean you can’t raise the issue of human rights.”
In the interview with VOA Mandarin, McGovern, who has been arrested three times protesting human rights violations in Sudan, said he is also concerned about human rights in Hong Kong, and China’s treatment of the ethnic minority group, the Uighurs.
‘We’re not perfect’
Listing hate crimes and attacks against members of the Muslim community, threats against Jewish community centers and hate crimes against the LGBTQ community, McGovern said he also worries about human rights in the United States, “so we’re not perfect.”
None of that, however, should lessen the attention paid to Tibet, McGovern said.
“I think the Chinese government thinks this issue will just go away. The Dalai Lama is in his 80s, and they think at some point he won’t be around and everybody will forget,” McGovern said.
But, he stressed, “we’re not going away, and this issue is not going away, and we’re going to keep on bringing it up over, and over, and over again until there’s some change.”
This story originated with VOA Mandarin.
DOOMED AMERICAN CHINA FANTASY – US HOUSE REPRESENTATIVE JIM McGOVERN CALLS FOR NEW US POLICY ON TIBET.US Policy on Tibet is not working. It will not work until and unless the US revises US Policy on Communist China. If Communism remains the ruling doctrine of China, no US Policy on Tibet will work. United States has no choice other than that of containing, engaging, confronting, and opposing China’s Communism.US Policy on Tibet is not working. It will not work until and unless the US revises US Policy on Communist China. If Communism remains the ruling doctrine of China, no US Policy on Tibet will work. United States has no choice other than that of containing, engaging, confronting, and opposing China’s Communism.